
DC911 document shows an almost six-minute delay during cardiac arrest
Mother comes to DC to get answers about her adult son's death

Looking for a quality used fire truck? Selling one? Visit our sponsor Command Fire Apparatus
Press conference with Stephania Clemans and Free Information Group
Seconds count when a person is in cardiac arrest. There’s no dispute about that fact. Yet, once again, DC911 delayed minutes – almost six, possibly more – before alerting paramedics to help William Ostertag after his heart stopped. This delay happened while the closest paramedics to the 28-year-old man sat inside the firehouse immediately next door to the apartment building where he collapsed. The medics and firefighters in Columbia Heights were unaware that help was needed less than 250 feet away.
Where DC911 was very slow on this call, the DC Fire and EMS Department moved rapidly once they learned of the emergency next door. From the time Paramedic Engine 11 and a paramedic supervisor were finally dispatched to the 911 call, until they reached Ostertag’s side and shocked his heart, only two minutes and 21 seconds elapsed. After multiple shocks and CPR, Ostertag’s heart began beating on its own. On the way to Washington Hospital Center, his heart stopped again. Medics restarted it. Despite these efforts by the DC Fire and EMS Department, Ostertag never regained consciousness. He died after 11 days in a coma.

This information about Will Ostertag’s collapse is not from inside sources or even radio traffic. It comes directly from DC Fire and EMS Department’s medical records. They were sent to Ostertag’s mother shortly after she filed a Freedom of Information Act request. A similar FOIA request took a little more time and some wrangling to get just a basic timeline out of the Office of Unified Communications/DC911.
Stephanie Clemans wants to know exactly what happened to her son after he collapsed while working out on a Peloton on November 3, 2024. Unfortunately, she has run into the same wall that other families have hit when dealing with OUC and the District of Columbia government. It’s OUC’s blanket policy of releasing 911 recordings only to the people who made the call.
The two 911 calls in this case are the only way to get definitive answers to the serious questions about DC911’s performance that are raised by the documents Clemans received. It’s also the only way she can get more details about the role of bystanders who tried to help her son. Clemans and her attorneys will speak at a press conference tomorrow about their efforts to get both the 911 calls and those answers. My focus in this article is on the questions and the delays.
Full disclosure
First, you should know that Stephanie Clemans, who lives in Kentucky, reached out to me last August looking for help in tracking down the critical moments following her son’s collapse. I am one of several people who have guided Clemans through her difficult journey. While I’ve explained the challenges in getting the information she wants and introduced her to some key people, the direction and decisions all come from Clemans.
My goal, as always, is to ultimately see major improvements at OUC. Real DC911 reform. Using what I’ve learned during these six years of advocacy journalism to help others navigate the system seems like the right thing to do.
Will Ostertag’s case is the sixteenth time in six years I’ve documented delays and mistakes made at DC911 where someone died. There is a potential seventeenth incident from December where multiple DC911 errors have been confirmed during another cardiac arrest. That call is not on my list yet because I have been unable to confirm whether the person was revived or died. These are just the deaths I know about.
If you’ve followed me long enough, you know that I share my opinion about DC911’s chronic poor performance. One thing I can guarantee you with this story and the other tragic DC911 cases is that those opinions are always based on the facts I’ve uncovered. The facts come first. So, here are the facts, outlining what we know and what we don’t yet know about OUC’s actions on November 3, 2024.
The Timeline
The timeline Stephanie Clemans received from OUC is a printout from the agency’s computer-aided dispatch (CAD) system. It outlines the various actions taken during the emergency by DC911 call-takers, dispatchers, and supervisors. Normally, OUC’s leadership holds the CAD reports very close. So close, that OUC Director Heather McGaffin refused to share the CAD report from the tragic District Dogs flood in 2023, despite a demand to see it from two council members.
The timeline after William Ostertag collapsed shows delays and raises a lot of questions about OUC’s actions. Here are the key moments.
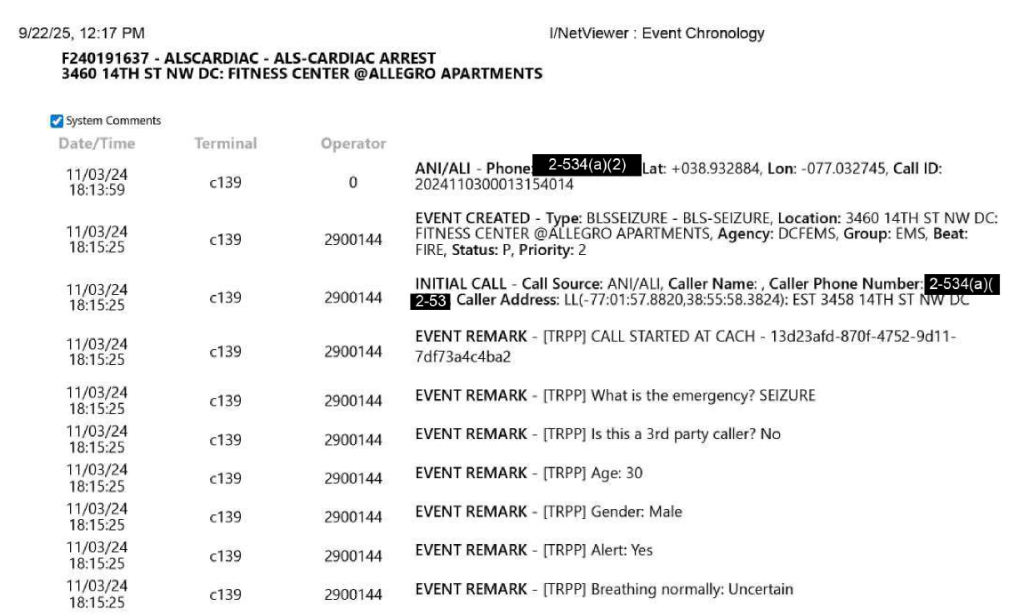
6:13:59 p.m. The initial 911 call was received at OUC. It came from the front desk at the Allegro apartments, on 14th Street NW where Ostertag lived.
6:15:25 p.m. An event was created in OUC’s dispatch computer. It’s unclear why it took 1 minute and 26 seconds for this to occur. This may not be a delay or mistake and may just be how OUC’s newer 911 call processing system, known as Power Phone Total Response, interacts with the agency’s older computer-aided dispatch system.
It appears that the 911 call-taker asked the normal series of standard questions prompted by Power Phone prior to this point. But all the answers populated in the computer at the same time, instead of in real time as they occurred.
From those answers, the type of incident was listed as “BLSSEIZURE”. This classification was key to the type of emergency care initially sent to Ostertag. The normal response to a seizure is a basic life support (BLS) ambulance and not paramedics. Paramedics are considered advanced life support (ALS).
The only way to determine if this was the correct call classification is to know exactly what the caller said. That’s why it’s so important for Stephanie Clemans to get the 911 recordings. The misclassification of EMS calls has been a chronic problem at OUC.
Current and former OUC workers who have reviewed this timeline for me believe at least one of the answers should have prompted an ALS response. That was when the caller said they were “uncertain” whether the patient was breathing normally.
6:15:42 p.m. Ambulance 28, from the firehouse on Connecticut Avenue NW in Cleveland Park, was the first unit dispatched. It was apparently the closest basic life support ambulance available at a little less than three miles away. Again, because of the seizure classification, the paramedics at the firehouse next door to Ostertag’s building were initially bypassed for this assignment.
6:16:00 p.m. For the first time, there was a notation saying the priority of the message was “critical”. There is an exclamation point inside of a red diamond with this notation and the subsequent mentions of the word “critical”. That is meant to get the attention of the dispatchers handling this call. It’s to alert them that something important has changed. A critical update.
6:16:14 p.m. A second 911 call was received about this incident, but no details were provided.
6:17:45 p.m. There was another note saying “critical”. A second priority alert to the dispatchers.
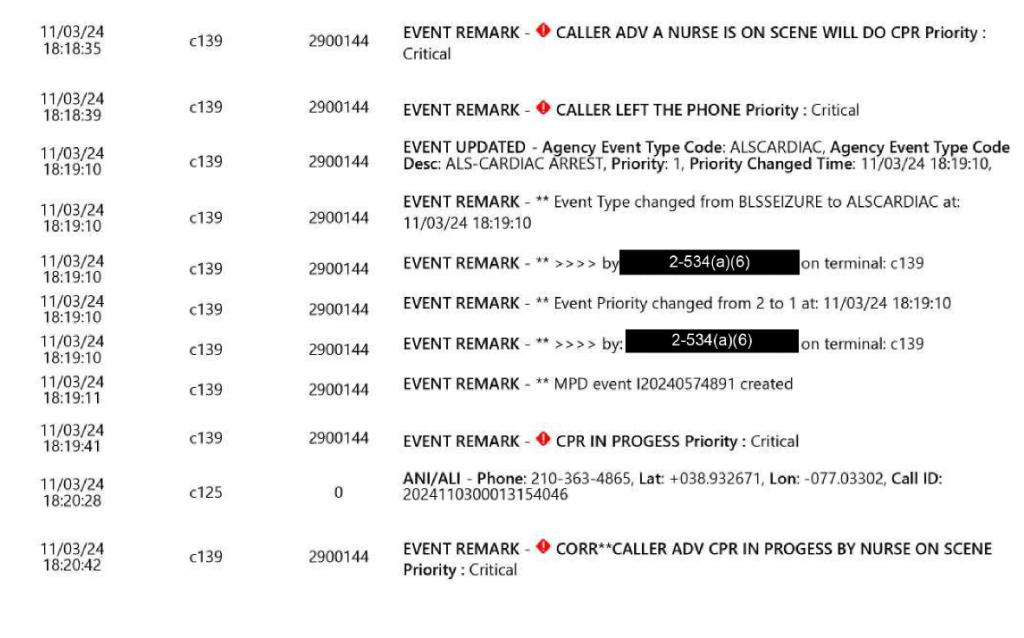
6:18:35 p.m. An entry said the caller advised a nurse was on the scene and she will do CPR with the message priority as “critical”.
6:19:10 p.m. The call type was changed from BLSSEIZURE to ALSCARDIAC, changing the priority of this incident from 2 to 1, the highest priority.
6:19:41 p.m. Another notation was made of CPR in progress with the message priority as “critical”.
6:21:45 p.m. There’s a notation saying the patient was not breathing, with the message priority as “critical”.
Despite all of these critical alerts that began at 6:16 p.m., no effort was made to dispatch paramedics. All the OUC insiders and other 911 experts I’ve talked with cite this significant delay as a major failure by the fire and EMS dispatch side of OUC. The issue of reading and reacting to updates, in particular those that are critical, is another chronic problem at OUC.
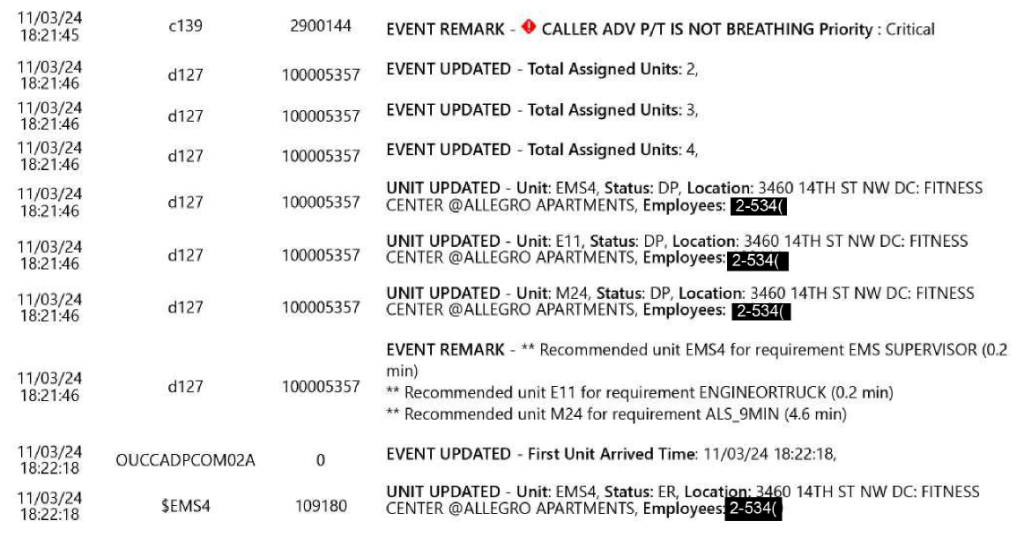
6:21:46 p.m. Finally, the response was upgraded to send Engine 11, EMS 4, and Medic 24, all advanced life support units. Unfortunately, this took five minutes and 46 seconds from the time of the first “critical” priority message. Or three minutes and 11 seconds from the time CPR was first mentioned. Or two minutes and 36 seconds from the time the call was changed to “ALSCARDIAC”.
All of this is extremely slow. These were seconds and minutes that William Ostertag or any sudden cardiac arrest victim can’t afford to lose.
6:22:18 p.m. Just 32 seconds after the paramedics and firefighters at the firehouse next door were alerted, they were on the scene and beginning their attempts to resuscitate William Ostertag. But at this point, it was eight minutes and 18 seconds after the first 911 call was received.
Finding answers
No one can say for certain if the outcome for William Ostertag would have been different if the proper emergency help had been sent sooner. But we can confidently say his chances of survival would have greatly improved if the paramedics who twice restarted his heart were dispatched eight, six, five, or three minutes earlier.
DC911 wasted precious time. While the initial call classification is still an open question, what happened from 6:16 p.m. on is very clear and very disturbing. OUC leadership has a long history of failing to be candid about its mistakes. Stephanie Clemans, like many before her, deserves answers. It’s shameful that she must hire lawyers and go to court to get those answers about her son’s final moments.



